



How to use Mirena
LEAFLET INCLUDED IN THE PACKAGE: INFORMATION FOR THE USER
Warning! Keep the leaflet, the information on the immediate packaging is in a foreign language!
Mirena (Mирена)
52 mg, 20 micrograms/24 hours, intrauterine therapeutic system
Levonorgestrel
Mirena and Mирена are the same trade names for the same drug written in Polish and Bulgarian languages.
You should carefully read the contents of the leaflet before using the drug, as it contains important information for the patient.
- You should keep this leaflet so that you can read it again if you need to.
- If you have any doubts, you should consult a doctor or pharmacist.
- This medicine has been prescribed specifically for you. Do not pass it on to others. The medicine may harm another person, even if their symptoms are the same as yours.
- If you experience any side effects, including any not listed in this leaflet, you should tell your doctor or pharmacist. See section 4.
Table of contents of the leaflet
1. What is Mirena and what is it used for
2. Important information before using Mirena
3. How to use Mirena
4. Possible side effects
5. How to store Mirena
6. Contents of the package and other information
1. What is Mirena and what is it used for
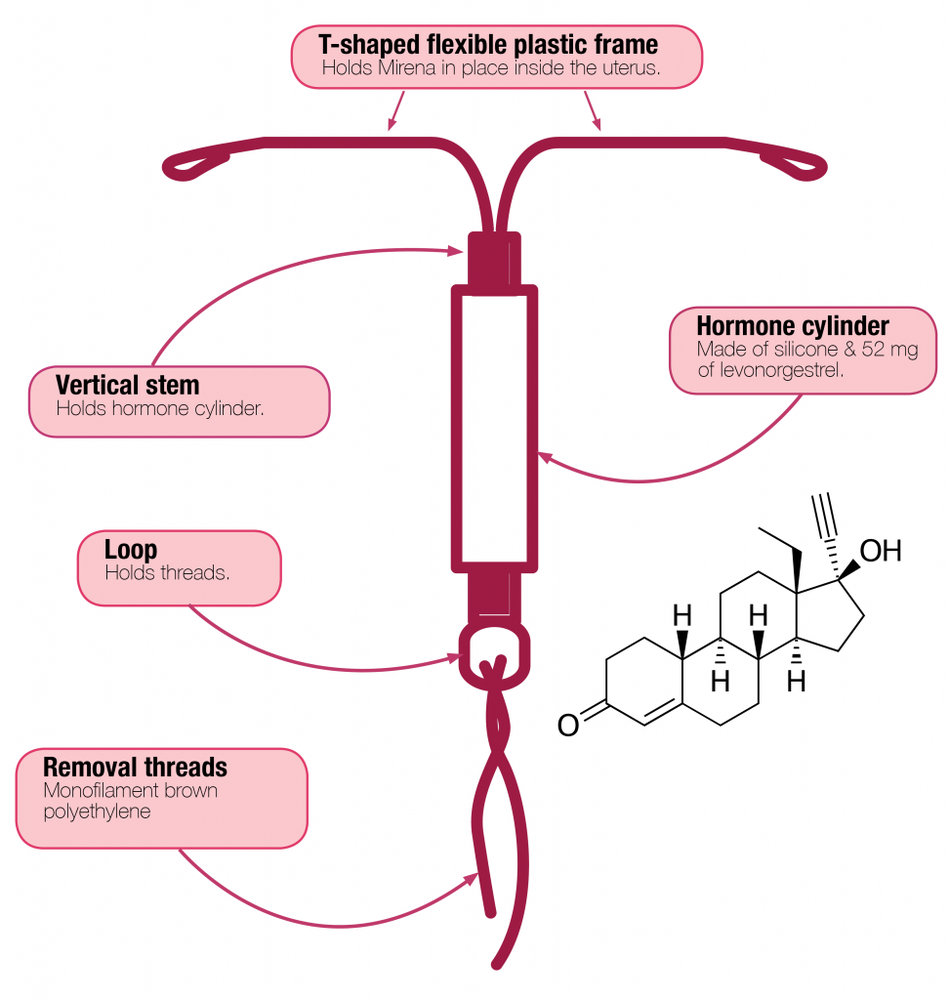
Mirena is an intrauterine therapeutic system in the shape of the letter "T", which, after insertion, releases the hormone - levonorgestrel into the uterus. The "T" shape ensures that the system fits into the uterus.
The vertical part of the white system contains a container with the drug containing levonorgestrel. Two brown threads are attached to the loop at the lower end of the system base, which serve to remove the system from the uterus.
Mirena is used to prevent pregnancy (contraceptive effect) and to treat excessive menstrual bleeding (of unknown origin).
Children and adolescents
Mirena is not indicated for use before the onset of menstruation (first menstrual bleeding).
2. Important information before using Mirena
General notes
Before using Mirena, the doctor will ask the patient a few questions about her health and the health of her close relatives.
This leaflet describes several situations in which it is necessary to remove Mirena or when the effectiveness of the system may be reduced. In such cases, you should either abstain from sexual intercourse or use additional non-hormonal contraceptive methods, such as a condom or other mechanical method. You should not use the calendar method or temperature measurement. They may prove to be ineffective, as Mirena affects monthly changes in body temperature and cervical mucus.
Mirena, like other hormonal contraceptives, does not protect against HIV (AIDS) or other sexually transmitted diseases.
Mirena should not be inserted if any of the following conditions are present:
- if the patient is allergic to levonorgestrel or any of the other ingredients of this medicine (listed in section 6)
- pregnancy or suspected pregnancy
- tumors whose growth is dependent on the action of progesterone, such as breast cancer
- existing or recurring inflammatory conditions of the pelvic organs (infections of the female reproductive organs)
- cervicitis
- lower genital tract infections
- postpartum endometritis
- infections of the uterus after abortion in the last 3 months
- conditions that promote the development of infection
- abnormal cervical cells
- cancer or suspected cancer of the cervix or uterus
- unexplained abnormal uterine bleeding
- abnormalities in the cervix or uterus, including fibroids, if they deform the uterus
- active liver disease or liver tumor
Warnings and precautions
Before starting to use the Mirena system, you should consult a doctor.
Consult a doctor who will decide whether to remove or not remove the Mirena system if any of the following conditions occur for the first time while using the Mirena system:
- migraine, asymmetric visual field defects or other symptoms that may be signs of transient cerebral ischemia (temporary blockage of blood flow to the brain)
- severe headache
- jaundice (yellowing of the skin, whites of the eyes, and/or nails)
- significant increase in blood pressure
- severe arterial disease, such as stroke or heart attack
- acute venous thromboembolic disease.
Mirena should be used with caution in women with congenital heart defects or heart valve defects that increase the risk of endocarditis.
In women with diabetes who use Mirena, blood glucose levels should be monitored.
Irregular bleeding may mask some symptoms and signs of endometrial polyps or cancer, and in these cases, diagnostic tests should be considered.
Medical examination/consultation
The examination before inserting Mirena may include a cervical smear as well as other tests, such as infection tests, including sexually transmitted diseases if necessary, pregnancy test. A gynecological examination should be performed to determine the position and size of the uterus.
Mirena is not a suitable contraceptive method for use as emergency contraception (post-coital contraception, emergency).
Infections
The applicator tube helps protect Mirena from microbial contamination during insertion. The Mirena applicator has been designed to reduce the risk of infection. Nevertheless, there is an increased risk of infection shortly after insertion and during the first month after insertion of Mirena. Pelvic inflammatory disease in women using Mirena is often associated with sexually transmitted diseases. The risk of infection increases with multiple sexual partners. Pelvic inflammatory disease must be properly treated, as it can affect fertility and increase the risk of ectopic pregnancy. Mirena should be removed in case of recurring inflammatory conditions of the endometrium or pelvic organs, if there are acute and severe inflammatory conditions or if they do not resolve after a few days of treatment.
In extremely rare cases, shortly after insertion of the intrauterine therapeutic system, severe infection or sepsis (a very severe infection that can be fatal) may occur.
You should contact your doctor immediately if you experience persistent lower abdominal pain, elevated body temperature, pain during sexual intercourse, and unusual vaginal bleeding.
Expulsion
Uterine contractions during menstrual bleeding may sometimes cause the system to move or be expelled. This is more likely if the woman is overweight at the time of insertion or if she has had heavy menstrual bleeding in the past. If the system is not in place, it may not work as intended, and the risk of pregnancy increases. Expulsion of the system results in loss of protection against pregnancy.
Possible symptoms of expulsion include vaginal bleeding or lower abdominal pain, but Mirena can also be expelled unnoticed. Since Mirena reduces the heaviness of menstrual bleeding, the intensity of these bleedings may be a sign of expulsion or displacement of the system.
It is recommended to check with your fingers (e.g., during bathing) whether the threads are in the correct position.
See also section 3 "How to use Mirena - Self-checking of the correct position of Mirena". If symptoms occur that may indicate expulsion of the system or if the threads cannot be felt in the cervix area, you should use other contraceptive methods (such as condoms) and contact your doctor.
Perforation of the uterus
Perforation or damage to the uterine wall may occur, most often during insertion, although it may only be detected later. Mirena that has ended up outside the uterus is not effective in preventing pregnancy and should be removed as soon as possible. To remove Mirena, surgery may be necessary. The risk of perforation is higher in breastfeeding women and within 36 weeks after delivery; this risk may also be increased in women with a permanently retroverted uterus (uterus tilted backwards). If you suspect perforation of the uterus, you should consult your doctor and inform them that you have Mirena, especially if it is not the doctor who inserted the system.
Possible signs and symptoms of perforation may include:
- severe pain (like menstrual cramps) or pain stronger than expected
- severe bleeding (after insertion)
- pain or bleeding that lasts longer than a few weeks
- sudden change in your periods
- pain during sexual intercourse
- inability to feel the threads of Mirena (see section 3 "How to use Mirena - Self-checking of the correct position of Mirena")
Ectopic pregnancy
Pregnancy during the use of Mirena is very unlikely. However, if a woman becomes pregnant while using Mirena, the likelihood of ectopic pregnancy is relatively increased. In about 1 in 1000 women who properly used Mirena, an ectopic pregnancy occurred within a year of use. This is less than in women who do not use any contraceptive methods (about 3 to 5 in 1000 women per year). In women who have had an ectopic pregnancy in the past, have had tubal surgery, or have had pelvic inflammatory disease, there is an increased risk of ectopic pregnancy. Ectopic pregnancy is a serious condition that requires immediate medical attention. Symptoms that may indicate an ectopic pregnancy and require immediate medical attention include:
- cessation of menstrual bleeding, followed by persistent bleeding or pain
- dull or very severe pain in the lower abdomen
- typical symptoms of pregnancy with concurrent bleeding and dizziness.
Fainting
Some women may experience dizziness after insertion of Mirena. This is a normal physiological reaction. The doctor will recommend resting for a while after insertion of Mirena.
Enlarged ovarian follicles surrounding the maturing egg cell in the ovary
The contraceptive properties of Mirena are related to its local action, so in women of childbearing age, menstrual cycles are usually ovulatory and ovulation occurs. Sometimes, the unruptured follicle does not regress for a while and may enlarge. In most cases, these enlarged follicles do not cause any symptoms, although they may cause pelvic pain or pain during intercourse. Such enlarged ovarian follicles usually resolve on their own, but may also require medical intervention.
Psychiatric disorders
Some women using hormonal contraceptives, including Mirena, have reported depression or low mood. Depression can be severe and sometimes lead to suicidal thoughts. If mood changes and symptoms of depression occur, you should contact your doctor as soon as possible for further medical advice.
Mirena and other medicines
Since the mechanism of action of Mirena is primarily local, taking other medicines should not increase the risk of pregnancy during the use of this system.
However, it is recommended that you tell your doctor about all the medicines you have taken recently, including those that are available without a prescription.
Pregnancy, breastfeeding, and fertility
Pregnancy
Mirena should not be used during pregnancy or if pregnancy is suspected.
Very rarely, a woman may become pregnant while Mirena is in place. However, if Mirena is displaced, contraceptive protection is reduced, and other contraceptive methods should be used until a doctor's visit.
During the use of Mirena, some women may experience cessation of menstrual bleeding after a while. Lack of menstrual bleeding does not always mean pregnancy. If menstrual bleeding has stopped and other signs of pregnancy occur (e.g., nausea, fatigue, breast tenderness), you should consult a doctor for an examination and a pregnancy test.
If a woman becomes pregnant while using Mirena, she should contact her doctor immediately to have the system removed. Removal may cause miscarriage. However, leaving Mirena in place during pregnancy may increase not only the risk of miscarriage but also the risk of preterm birth. If Mirena cannot be removed, you should discuss the benefits and risks associated with continuing the pregnancy with your doctor. If the pregnancy is maintained, it should be monitored by a doctor, and you should immediately inform your doctor if symptoms such as abdominal cramps, abdominal pain, or fever occur.
Mirena contains a hormone called levonorgestrel, and there have been single reports of its effect on the genital organs of girls exposed to levonorgestrel released from an intrauterine device remaining in the uterus.
Breastfeeding
Mirena can be used during breastfeeding. Levonorgestrel passes into breast milk in small amounts (about 0.1% of the levonorgestrel dose may pass into the child's body through breast milk). After 6 weeks postpartum, the use of Mirena does not have any harmful effect on the growth and development of the child. It has not been found that progestogen-only contraceptives affect the amount and quality of milk.
Hormonal contraception is not recommended as the first choice during breastfeeding; only non-hormonal contraceptive methods are recommended. Progestogen-only contraceptive methods, such as Mirena, are second-choice methods. The daily dose and blood levonorgestrel levels are lower than with other hormonal contraceptive methods.
Fertility
Removal of Mirena restores a woman's normal fertility.
If you are pregnant or breastfeeding, or suspect that you are pregnant or plan to become pregnant, you should consult your doctor or pharmacist before taking this medicine.
Driving and using machines
No effects of Mirena on the ability to drive and use machines have been found.
Important information about some of the ingredients of Mirena:
The T-shaped skeleton of Mirena contains barium sulfate, which allows the system to be visualized during X-ray examination.
3. How to use Mirena
Efficacy of Mirena
The contraceptive efficacy of Mirena is the same as that of the most effective copper-containing intrauterine device. In clinical trials, about 2 pregnancies per 1000 women using Mirena were found in the first year.
In the treatment of excessive menstrual bleeding of unknown origin, Mirena reduces the severity of bleeding after just 3 months of use. In some women, it is possible to completely stop menstruation.
When should Mirena be inserted?
Starting to use Mirena
- Before inserting Mirena, you should make sure that the patient is not pregnant.
- Mirena should be inserted within 7 days of the start of menstrual bleeding. If Mirena is inserted during these days, the system will work immediately and prevent pregnancy.
- If Mirena cannot be inserted within 7 days of the start of menstrual bleeding or if menstruation occurs at an unpredictable time, the system can be inserted on any day. In this case, you should not have sexual intercourse without using contraception from the last menstrual bleeding and before insertion, and you should have a negative pregnancy test result. Additionally, Mirena may not prevent pregnancy immediately and reliably. Therefore, you should use a barrier method of contraception (such as condoms) or abstain from sexual intercourse for 7 days after insertion of Mirena.
Starting to use Mirena after childbirth
- Mirena can be inserted after the birth of a child, when the uterus has returned to its normal size, but not earlier than 6 weeks after childbirth (see section 2: "Important information before using Mirena - Perforation of the uterus").
- See also "Starting to use Mirena" above to find out what else you need to know about the timing of system insertion.
Starting to use Mirena after abortion
Mirena can be inserted immediately after an abortion in the first trimester, provided that there is no infection of the genital tract. Mirena will then work immediately.
Replacing Mirena
Mirena can be replaced with a new one on any day of the menstrual cycle. Mirena will then work immediately.
Changing from another contraceptive method (e.g., combined hormonal contraceptives, implant)
- Mirena can be inserted immediately if there is justified certainty that the patient is not pregnant.
- If more than 7 days have passed since the start of menstrual bleeding, you should abstain from sexual intercourse or use additional contraceptive protection for the next 7 days.
How to insert Mirena
Mirena should only be inserted by a doctor or other qualified medical personnel with experience in inserting the system.
After a gynecological examination, a speculum is inserted into the vagina and the cervix is rinsed with an antiseptic solution. The intrauterine system is then inserted into the uterus through a thin, flexible plastic tube (applicator). If necessary, the cervix can be locally anesthetized before insertion.
Some people may experience pain and dizziness after insertion of the system. If these symptoms do not
resolve within half an hour in a patient who remains in a lying position, it may indicate that the system has been
inserted incorrectly. An examination should be performed and the system removed if necessary.
After insertion of Mirena, the patient should receive a reminder card from the doctor, which will be used to record the dates of follow-up examinations. This card should be brought to every scheduled visit.
When to contact a doctor
The doctor should check the presence of the system within 4 to 12 weeks after its insertion and then regularly check the presence of the system at least once a year. The doctor will determine individually how often and what follow-up examinations should be performed. You should bring the reminder card for the patient, received from the doctor, to every scheduled visit. Additionally, you should contact your doctor if:
- the threads in the vagina are not palpable
- the lower part of the system is palpable
- you suspect that you are pregnant
- you experience persistent abdominal pain, fever, or unusual vaginal discharge
- you or your partner experience pain or discomfort during sexual intercourse
- you experience sudden changes in your menstrual cycle (e.g., scanty or absent menstrual bleeding, followed by persistent bleeding or pain, or sudden heavy bleeding)
- you experience other health problems, such as migraine headaches or severe headaches that recur, sudden vision problems, jaundice, or increased blood pressure
- any of the conditions listed in section 2 "Important information before using Mirena" occur.
Remind your doctor that you have Mirena, especially if it is not the doctor who inserted the system.
Duration of use of Mirena
Mirena prevents pregnancy (has a contraceptive effect) for 8 years after insertion. If the patient uses Mirena for this purpose, the system should be removed or replaced no later than 8 years after insertion.
Mirena is effective for 5 years after insertion in the treatment of excessive menstrual bleeding (of unknown origin). If the patient uses Mirena for this purpose, the system should be removed or replaced when excessive menstrual bleeding returns or no later than 8 years after insertion. If the patient wishes, a new system can be inserted after removal of the previous one.
If you want to remove Mirena to become pregnant or for other reasons
The doctor can easily remove the system at any time, and then it is possible to become pregnant.
Removal of the system is usually painless. After removal of Mirena, fertility returns.
Continuing contraception after removal of the system
If you do not plan to become pregnant, Mirena should not be removed after the 7th day of the menstrual cycle (unless other contraceptive methods are used, such as condoms, for at least 7 days before removal of the system). If you have irregular menstruation (periods) or do not have menstruation, you should use mechanical contraceptive methods for at least 7 days before removal of the system and until menstruation returns. You can also have a new system inserted immediately after removal of the previous one, and in this case, no additional protection is required. If you do not want to continue using the same method, you should ask your doctor for advice on other proven contraceptive methods.
Can you become pregnant after stopping the use of Mirena
Yes. Removal of Mirena does not disrupt fertility. You can become pregnant during the first menstrual cycle after removal of Mirena.
Does Mirena affect menstrual bleeding
Mirena affects the menstrual cycle. The system can cause various changes in menstruation, such as spotting (minor blood loss), shorter or longer bleeding, scanty or heavy bleeding, or its absence.
In many women, during the first 3 to 6 months after insertion of Mirena, in addition to menstrual bleeding, frequent spotting or minor bleeding occurs. In some women, menstrual bleeding may become heavier or longer than usual. You should then inform your doctor, especially if these symptoms do not resolve.
Generally, it is possible to gradually reduce the number of days of bleeding and the amount of blood lost each month. In some women, menstruation may eventually stop completely. Since Mirena usually reduces the heaviness of menstrual bleeding, many women experience an increase in hemoglobin levels in the blood.
After removal of the system, menstruation returns to normal.
Is the absence of menstrual bleeding a normal condition
Yes, when using Mirena. The absence of menstruation is a sign of the effect of the hormone on the endometrium. There is no monthly thickening of the endometrium. Therefore, there is nothing that would be naturally shed with menstrual blood. This does not have to be a sign of menopause or pregnancy. Hormone levels remain normal.
In fact, the absence of menstruation can be a great benefit for a woman's health.
Diagnosing pregnancy
Becoming pregnant while using Mirena is unlikely, even if menstrual bleeding does not occur.
If menstrual bleeding has not occurred for 6 weeks and this causes concern, a pregnancy test can be performed. If the result is negative, there is no need for further testing, unless other symptoms of pregnancy occur, such as nausea, fatigue, or breast tenderness.
Can Mirena cause pain or discomfort
Some women experience pain (like menstrual cramps) for a few weeks after insertion of the system. You should consult your doctor or clinic again if you experience severe pain or if pain persists for more than 3 weeks after insertion of Mirena.
Effect of Mirena on sexual intercourse
Neither the patient nor the partner should feel the system during sexual intercourse. If they do feel it, they should avoid sexual intercourse until the doctor checks whether the system is still in the correct position.
How soon after insertion of the system can you have sexual intercourse
To allow the body to rest, it is recommended to wait about 24 hours after insertion of the system before having sexual intercourse. Nevertheless, Mirena prevents pregnancy immediately after insertion.
Using tampons or menstrual cups
It is recommended to use sanitary pads. If you use tampons or menstrual cups, you should change them carefully so as not to pull on the threads of Mirena. If you think that Mirena has been displaced from its correct position (see "When to contact a doctor" with possible symptoms), you should avoid sexual intercourse or use mechanical contraception (such as condoms) and contact your doctor.
What happens when Mirena is expelled
Rarely, but it is possible, that Mirena may be expelled without the patient's knowledge during menstrual bleeding. If menstrual bleeding is heavier than usual, it may mean that Mirena has been expelled through the vagina. It is also possible that Mirena is partially expelled from the uterus (the patient and partner may notice this during sexual intercourse). If Mirena is completely or partially expelled, it does not protect against pregnancy.
Self-checking of the correct position of Mirena
A woman can check herself whether the threads of the system are in the correct position. To do this, she should carefully insert her finger into the vagina and check the presence of the threads near the cervix.
Do not pull on the threads, as this can cause unintentional removal of the system. If the threads are not felt, it may mean that the system has been expelled from the uterus or that the uterus has been perforated. In this case, you should use mechanical contraception (such as condoms) and contact your doctor.
4. Possible side effects
Like all medicines, Mirena can cause side effects, although not everybody gets them.
In addition to the possible side effects listed in other sections (e.g., section 2 "Important information before using Mirena"), the following side effects are possible, divided by body system and frequency of occurrence:
Very common:may occur in 1 in 10 patients
Disorders of the reproductive system and breast
- uterine or vaginal bleeding, including spotting, infrequent menstruation, or absence of menstruation
- mild ovarian cysts (see section 2: "enlarged ovarian follicles")
Common:may occur in 1 to 10 in 100 patients
Psychiatric disorders
- depressed mood or depression
- nervousness
- decreased libido
Nervous system disorders
- headache
Vascular disorders
- dizziness
Gastrointestinal disorders
- abdominal pain
- nausea
Skin and subcutaneous tissue disorders
- acne
Musculoskeletal, connective tissue, and bone disorders
- back pain
Reproductive system and breast disorders
- pelvic pain
- painful menstruation
- leukorrhea
- vulvovaginitis
- breast tenderness
- breast pain
- expulsion of the intrauterine therapeutic system
Diagnostic tests
- weight gain
Uncommon:may occur in 1 to 10 in 1000 patients
Nervous system disorders
- migraine
Gastrointestinal disorders
- abdominal distension
Skin and subcutaneous tissue disorders
- hirsutism (male-type hair growth in women)
- hair loss (alopecia)
- pruritus (severe itching)
- rash (skin inflammation)
- chloasma (yellow-brown spots on the skin) or intense skin discoloration
Reproductive system and breast disorders
- perforation (puncture) of the uterus
- pelvic inflammatory disease (infection of the upper female reproductive organs, organs above the cervix)
- endometritis (inflammation of the uterine lining)
- cervicitis - normal smear class II Papanicolaou in cytological examination (cervicitis)
General disorders and administration site conditions
- edema
Rare:may occur in 1 to 10 in 10,000 patients
Skin and subcutaneous tissue disorders
- urticaria
- angioedema
If a woman becomes pregnant while using Mirena, there is a likelihood that the pregnancy will be ectopic (see section 2: "Ectopic pregnancy").
After insertion of the intrauterine therapeutic system, cases of sepsis (a very severe infection that can be fatal) have been reported.
Reporting side effects
If you experience any side effects, including any not listed in this leaflet, you should tell your doctor or pharmacist.
Side effects can be reported directly to the Department of Drug Safety Monitoring of the Office for Registration of Medicinal Products, Medical Devices, and Biocidal Products, Al. Jerozolimskie 181C, 02-222 Warsaw, Tel.: +48 22 49 21 301, Fax: +48 22 49 21 309, website: https://smz.ezdrowie.gov.pl .
Side effects can also be reported to the marketing authorization holder.
Reporting side effects will help to gather more information on the safety of the medicine.
5. How to store Mirena
Store out of sight and reach of children.
Storage: No special storage precautions are required.
Do not insert Mirena after the expiration date stated on the packaging. The expiration date refers to the last day of the specified month.
Medicines should not be disposed of via wastewater or household waste. You should ask your pharmacist how to dispose of medicines that are no longer needed. This will help protect the environment.
6. Contents of the package and other information
What Mirena contains
- The active substance of Mirena is levonorgestrel. One intrauterine therapeutic system contains 52 mg of levonorgestrel.
- The other ingredients of Mirena are: polydimethylsiloxane elastomer; polydimethylsiloxane tubing (contains anhydrous colloidal silica); T-body (consisting of: polyethylene containing 20-24% barium sulfate); threads (consisting of: polyethylene, iron oxides (E 172) below 1%).
What Mirena looks like and what the package contains
Package size: one sterile packaged intrauterine therapeutic system for intrauterine use.
To obtain more detailed information, you should contact your doctor, the marketing authorization holder, or the parallel importer.
Marketing authorization holder in Bulgaria, the country of export:
Bayer AG
Kaiser-Wilhelm-Allee 1
51373 Leverkusen
Germany
Manufacturer
Bayer Oy
Pansiontie 47
20210 Turku
Finland
Parallel importer:
Medezin Sp. z o.o.
ul. Zbąszyńska 3
91-342 Łódź
Repackaged by:
Medezin Sp. z o.o.
ul. Zbąszyńska 3
91-342 Łódź
Marketing authorization number in Bulgaria, the country of export: 9800344
Parallel import authorization number: 2/24
Date of approval of the leaflet: 04.01.2024
[Information about the trademark]
- Country of registration
- Active substance
- Prescription requiredYes
- Marketing authorisation holder (MAH)Bayer AG
- This information is for reference only and does not constitute medical advice. Always consult a licensed doctor before taking any medication. Oladoctor is not responsible for medical decisions based on this content.
- Alternatives to MirenaDosage form: System, 19.5 mg/systemActive substance: plastic IUD with progestogenManufacturer: BAYER OyPrescription requiredDosage form: System, 52 mg (20 mcg/24h)Active substance: plastic IUD with progestogenPrescription requiredDosage form: System, 52 mg (20 mcg/24 h)Active substance: plastic IUD with progestogenPrescription required
Alternatives to Mirena in other countries
The best alternatives with the same active ingredient and therapeutic effect.
Alternative to Mirena in Ukraine
Alternative to Mirena in Spain
Online doctors for Mirena
Discuss dosage, side effects, interactions, contraindications, and prescription renewal for Mirena – subject to medical assessment and local rules.

Get updates and exclusive offers
Be the first to know about new services, marketplace updates, and subscriber-only promos.

