


NOVYNETTE 0.02 mg/0.15 mg Tablets

Prescription review online
A doctor will review your case and decide whether a prescription is medically appropriate.

Talk to a doctor about this medicine
Discuss your symptoms and possible next steps in a quick online consultation.


How to use Novinette
Contents of the leaflet
- Leaflet attached to the packaging: patient information
- Note! The leaflet should be kept. Information on the immediate packaging in a foreign language.
- Novynette (Desorelle 20)
- 02 mg + 0.15 mg, coated tablets
- What is Novynette and what is it used for
- Important information before using Novynette
- General notes
- When not to use Novynette
- Warnings and precautions
- The doctor should be told if the patient has any of the following conditions.
- BLOOD CLOTS
- It should be remembered that the total risk of harmful blood clots caused by Novynette is small.
- HOW TO RECOGNIZE BLOOD CLOTS
- BLOOD CLOTS IN VEINS
- What can happen if blood clots form in a vein?
- When is the risk of blood clots in a vein the highest?
- What affects the risk of blood clots in veins?
- Factors that increase the risk of blood clots in veins
- BLOOD CLOTS IN ARTERIES
- What can happen if blood clots form in an artery?
- Factors that increase the risk of blood clots in arteries
- Tablet and cancer
- Psychiatric disorders
- Irregular bleeding
- What to do if withdrawal bleeding does not occur during the withdrawal week
- Children and adolescents
- Novynette and other drugs
- Lab tests
- Pregnancy and breastfeeding
- Driving and using machines
- Novynette contains lactose monohydrate
- How to use Novynette
- Possible Side Effects
- How to Store Novynette
- Package Contents and Other Information
Leaflet attached to the packaging: patient information
Note! The leaflet should be kept. Information on the immediate packaging in a foreign language.

Not sure if this medicine is right for you?
Discuss your symptoms and treatment with a doctor online.
Novynette (Desorelle 20)
0.02 mg + 0.15 mg, coated tablets
Ethinylestradiol + Desogestrel
Novynette and Desorelle 20 are different trade names for the same drug.
Important information about combined hormonal contraceptives:
- If used correctly, they are one of the most reliable, reversible methods of contraception.
- They slightly increase the risk of blood clots in veins and arteries, especially in the first year of use or after resuming use after a break of 4 weeks or more.
- Caution should be exercised and a doctor should be consulted if the patient suspects that symptoms of blood clots have occurred (see section 2 "Blood clots").
The leaflet should be read carefully before using the drug, as it contains important information for the patient
- The leaflet should be kept so that it can be re-read if necessary.
- In case of any doubts, a doctor or pharmacist should be consulted.
- The drug has been prescribed to a specific person. It should not be given to others. The drug may harm another person.
- If the patient experiences any side effects, including any side effects not listed in this leaflet, they should tell their doctor or pharmacist. See section 4.
Table of contents of the leaflet
- 1. What is Novynette and what is it used for
- 2. Important information before using Novynette
- 3. How to use Novynette
- 4. Possible side effects
- 5. How to store Novynette
- 6. Package contents and other information

Started taking the medicine and have questions?
Discuss your symptoms and treatment with a doctor online.
1. What is Novynette and what is it used for
Novynette is a combined oral contraceptive containing ethinylestradiol (estrogen) and desogestrel (progestogen) in small doses. The mechanism of action of Novynette is based on the inhibition of ovulation and changes in the consistency of cervical mucus. When used correctly, Novynette provides an effective and reversible method of contraception. However, in certain situations, its contraceptive effectiveness may be reduced or the need to discontinue the drug may arise (see section 2). It is then recommended to either abstain from sexual intercourse or use other contraceptive methods, such as condoms or spermicides.
It should be remembered that combined oral contraceptives, such as Novynette, do not protect
against infection with sexually transmitted diseases (such as AIDS).Only the use of condoms has a protective effect.
2. Important information before using Novynette
General notes
Before starting to take Novynette, you should familiarize yourself with the information about blood clots (thrombosis) in section 2. It is especially important to familiarize yourself with the symptoms of blood clots (see section 2 "Blood clots").
Novynette should not be used to delay the start of bleeding.
In exceptional cases, when there is a need to delay the start of bleeding, you should consult a doctor.
Before starting to use Novynette, the doctor will ask the patient a few questions about her health and the health of her close relatives. The doctor will also measure blood pressure and, depending on the individual case, may also perform some other tests.
When not to use Novynette
Novynette should not be used if the patient has any of the following conditions. If the patient has any of the following conditions, they should inform their doctor. The doctor will discuss with the patient which other contraceptive method will be more suitable.
- If the patient is allergic to ethinylestradiol or desogestrel or any of the other ingredients of this drug (listed in section 6); may cause itching, rash or swelling;
- If the patient currently has (or has ever had) a blood clot in the blood vessels of the legs (deep vein thrombosis), lungs (pulmonary embolism), or other organs;
- If the patient knows that she has disorders that affect blood clotting - such as protein C deficiency, protein S deficiency, antithrombin III deficiency, factor V Leiden, or antiphospholipid antibodies;
- If the patient requires surgery or will be immobilized for a long time (see section "Blood clots");
- If the patient has had a heart attack or stroke;
- If the patient has (or has had in the past) angina pectoris (a disease that causes severe chest pain and may be the first symptom of a heart attack) or transient ischemic attack (transient stroke symptoms);
- If the patient has any of the following diseases, which may increase the risk of arterial thrombosis:
- severe diabetes with vascular damage,
- very high blood pressure,
- very high levels of fats in the blood (cholesterol or triglycerides),
- a disease called hyperhomocysteinemia;
- If the patient has (or has had in the past) a type of migraine called "migraine with aura";
- If the patient has (or has had in the past) pancreatitis;
- If the patient has (or has had in the past) liver disease, and liver function has not returned to normal;
- If the patient has (or has had in the past) liver tumors;
- If the patient has (or has had in the past) or suspects breast or genital cancer;
- If the patient has unexplained vaginal bleeding;
- If the patient has an enlarged endometrium (abnormal growth of the uterine lining);
- If the patient is or may be pregnant.
Novynette should not be used in patients with hepatitis C and taking medicinal products containing ombitasvir/paritaprevir/ritonavir, dasabuvir, glecaprevir/pibrentasvir, or sofosbuvir/velpatasvir/voxilaprevir (see also section "Novynette and other drugs").
Warnings and precautions
Before starting to use Novynette, you should discuss it with your doctor or pharmacist.
In some cases, you should be particularly careful when using Novynette or other combined hormonal contraceptives, and regular visits to the doctor may be necessary.
The doctor should be told if the patient has any of the following conditions.
If these symptoms occur or worsen while using Novynette, the doctor should also be told.
- if the patient experiences symptoms of angioedema, such as swelling of the face, tongue, and/or throat, and/or difficulty swallowing or hives, potentially with breathing difficulties, the doctor should be contacted immediately. Estrogen-containing products may cause or worsen symptoms of hereditary or acquired angioedema.
- if the patient smokes;
- if the patient is overweight;
- if the patient has high blood pressure;
- if the patient has heart valve defects or heart rhythm disorders;
- if the patient has superficial thrombophlebitis (thrombotic inflammation of the veins under the skin);
- if the patient has Crohn's disease or ulcerative colitis (chronic inflammatory bowel diseases);
- if the patient has systemic lupus erythematosus (a disease that affects the body's natural defense system);
- if the patient has hemolytic uremic syndrome (a blood clotting disorder that causes kidney failure);
- if the patient has sickle cell anemia (a hereditary disease of red blood cells);
- if the patient has been diagnosed with high levels of fats in the blood (hypertriglyceridemia) or has a family history of this disease. Hypertriglyceridemia is associated with an increased risk of developing pancreatitis;
- if the patient requires surgery or will be immobilized for a long time (see section "Blood clots".
- if the patient has recently given birth, she is at increased risk of blood clots. The doctor should be consulted to determine how soon after childbirth Novynette can be started;
- if the patient has varicose veins;
- if breast cancer has occurred or occurred in the patient's close relatives;
- if the patient has liver or gallbladder disease;
- if the patient has diabetes;
- if the patient has depression or mood changes;
- if the patient has epilepsy (see section "Novynette and other drugs"); When to contact a doctor?
The doctor should be contacted immediately
- if the patient notices possible symptoms of blood clots, which may indicate that the patient has blood clots in the leg (deep vein thrombosis), blood clots in the lungs (pulmonary embolism), heart attack, or stroke (see below "Blood clots".
To find a description of the serious side effects listed, see "How to recognize blood clots".
- if the patient has a disease that first appeared during pregnancy or while using sex hormones [e.g. hearing loss, a blood disease called porphyria, herpes gestationis (a skin rash with blisters during pregnancy), Sydenham's chorea (a nervous system disease in which there are involuntary movements of the body)];
- if the patient has or has had chloasma (golden-brown pigment spots, so-called pregnancy spots, especially on the face). In this case, direct exposure to sunlight or ultraviolet radiation should be avoided.
BLOOD CLOTS
The use of combined hormonal contraceptives, such as Novynette, is associated with an increased risk of blood clots, compared to not using hormone therapy. In rare cases, a blood clot can block a blood vessel and cause serious complications.
Blood clots can occur
- in veins (hereinafter referred to as "venous thromboembolism" or "venous thromboembolic disease"),
- in arteries (hereinafter referred to as "arterial thromboembolism" or "arterial thromboembolic disease"). Not all blood clots are completely resolved after treatment. In rare cases, the effects of a blood clot can be permanent or, very rarely, fatal.
It should be remembered that the total risk of harmful blood clots caused by Novynette is small.
HOW TO RECOGNIZE BLOOD CLOTS
The doctor should be contacted immediately if any of the following symptoms are noticed.
Is the patient experiencing any of these symptoms?
Why is the patient likely to be suffering?
- swelling of the leg or swelling along a vein in the leg or foot, especially if Deep vein thrombosis is accompanied by:
- pain or tenderness in the leg, which may only be felt when standing or walking,
- increased temperature in the affected leg,
- change in skin color of the leg, e.g. pallor, redness, or cyanosis. Pulmonary embolism
- sudden unexplained shortness of breath or rapid breathing;
- sudden unexplained cough, which may be accompanied by coughing up blood;
- sharp chest pain, which may worsen with deep breathing;
- severe dizziness or fainting;
- rapid or irregular heartbeat;
- severe abdominal pain.
If the patient is unsure, they should contact a doctor, as some of these symptoms, such as cough or shortness of breath, may be mistaken for milder conditions, such as a respiratory infection (e.g. a cold).
Symptoms usually occur in one eye:
- sudden loss of vision or,
- painless vision disturbances, which can lead to loss of vision. Retinal vein thrombosis (blood clot in the eye)
| Myocardial infarction |
| Stroke |
| Blood clots blocking other blood vessels |
BLOOD CLOTS IN VEINS
What can happen if blood clots form in a vein?
- The use of combined hormonal contraceptives is associated with an increased risk of blood clots in the veins (venous thromboembolism). Although these side effects are rare, they most often occur in the first year of using combined hormonal contraceptives.
- If blood clots form in the veins of the leg or foot, it can lead to the development of deep vein thrombosis.
- If a blood clot moves from the leg and settles in the lungs, it can cause pulmonary embolism.
- In very rare cases, a blood clot can form in another organ, such as the eye (retinal vein thrombosis).
When is the risk of blood clots in a vein the highest?
The risk of forming blood clots in a vein is highest during the first year of using combined hormonal contraceptives for the first time. The risk may also be higher when resuming the use of combined hormonal contraceptives (the same or a different drug) after a break of 4 weeks or more.
After the first year, the risk decreases, although it is always higher compared to not using combined hormonal contraceptives.
If the patient stops using Novynette, the risk of blood clots returns to normal within a few weeks.
What affects the risk of blood clots in veins?
The risk depends on the natural risk of venous thromboembolism and the type of combined hormonal contraceptive used.
The total risk of blood clots in the legs or lungs associated with Novynette is small.
- In a year, about 2 out of 10,000 women who do not use combined hormonal contraceptives and are not pregnant will develop blood clots.
- In a year, about 5-7 out of 10,000 women who use combined hormonal contraceptives containing levonorgestrel, norethisterone, or norgestimate will develop blood clots.
- In a year, about 9-12 out of 10,000 women who use combined hormonal contraceptives containing desogestrel, such as Novynette, will develop blood clots.
- The risk of blood clots depends on the patient's individual medical history (see "Factors that increase the risk of blood clots in veins", below).
| Risk of blood clots in a year | |
| Women who do not use combined hormonal tablets, patches, vaginal systems, and are not pregnant. | About 2 out of 10,000 women |
| Women using combined hormonal contraceptive tablets containing levonorgestrel, norethisterone, or norgestimate. | About 5-7 out of 10,000 women |
| Women using Novynette. | About 9-12 out of 10,000 women |
Factors that increase the risk of blood clots in veins
The risk of blood clots associated with Novynette is small, but some factors can increase this risk. The risk is higher:
- if the patient is significantly overweight (body mass index (BMI) over 30 kg/m);
- if someone in the patient's close family has had blood clots in the legs, lungs, or other organs at a young age (e.g. under 50 years old). In this case, the patient may have hereditary blood clotting disorders;
- if the patient needs to have surgery, is immobilized for a long time due to injury or illness, or has a leg in a cast. It may be necessary to temporarily stop using Novynette for a few weeks before surgery or immobilization. If the patient must stop using Novynette, they should ask their doctor when they can resume using the drug;
- with age (especially over 35 years old);
- if the patient has recently given birth.
The risk of blood clots increases with the number of risk factors present in the patient.
Long-haul flights (>4 hours) may temporarily increase the risk of blood clots, especially if the patient has another risk factor.
It is essential to tell the doctor if any of these risk factors are present, even if the patient is unsure. The doctor may decide to stop using Novynette.
The doctor should be informed if any of the above conditions change while using Novynette, e.g. if someone in the patient's close family is diagnosed with thrombosis without a known cause or if the patient gains significant weight.
BLOOD CLOTS IN ARTERIES
What can happen if blood clots form in an artery?
Similarly to blood clots in veins, blood clots in arteries can have serious consequences, such as a heart attack or stroke.
Factors that increase the risk of blood clots in arteries
It is essential to emphasize that the risk of heart attack or stroke associated with Novynette is very small, but some factors can increase this risk. The risk is higher:
- with age (over approximately 35 years old);
- if the patient smokes. During the use of a hormonal contraceptive like Novynette, it is recommended to quit smoking. If the patient cannot quit smoking and is over 35 years old, the doctor may recommend using a different type of contraception;
- if the patient is overweight;
- if the patient has high blood pressure;
- if someone in the patient's close family has had a heart attack or stroke at a young age (under 50 years old). In this case, the patient may also be at increased risk of having a heart attack or stroke;
- if the patient or someone in their close family has been diagnosed with high levels of fats in the blood (cholesterol or triglycerides);
- if the patient has migraines, especially migraines with aura;
- if the patient has heart disease (valve damage, heart rhythm disorder called atrial fibrillation);
- if the patient has diabetes. If the patient has more than one of the above conditions or if any of them are severe, the risk of blood clots may be even higher.
The doctor should be informed if any of the above conditions change while using Novynette, e.g. if the patient starts smoking, someone in the patient's close family is diagnosed with thrombosis without a known cause, or if the patient gains significant weight.
Tablet and cancer
Women using oral contraceptives have a slightly higher incidence of breast cancer than women of the same age who do not use them. This small increase in the incidence of breast cancer disappears gradually within 10 years of stopping the use of oral contraceptives. It is not known whether this difference is caused by the use of oral contraceptives. It may be related to the fact that women using oral contraceptives are more likely to have medical examinations and breast cancer is diagnosed earlier in them.
Women using oral contraceptives have been reported to have, in rare cases, benign liver tumors, and in even rarer cases, malignant liver tumors. If the patient experiences unusual, severe abdominal pain, they should contact their doctor.
Psychiatric disorders
Some women using hormonal contraceptives, including Novynette, have reported depression or low mood. Depression can be severe and sometimes lead to suicidal thoughts. If mood changes and symptoms of depression occur, the patient should contact their doctor as soon as possible for further medical advice.
Irregular bleeding
During the first few months of taking Novynette, unexpected bleeding (bleeding outside the withdrawal week) may occur. If such bleeding persists for longer than a few months or starts after a few months, the doctor should be consulted to determine the cause.
What to do if withdrawal bleeding does not occur during the withdrawal week
If all the tablets have been taken correctly, there has been no vomiting or severe diarrhea, and no other drugs have been taken, it is very unlikely that the woman is pregnant.
If the expected withdrawal bleeding does not occur for two consecutive times, it may indicate pregnancy. The doctor should be contacted immediately. The next pack of Novynette should only be started when the patient is sure she is not pregnant.
Children and adolescents
The safety and efficacy of using Novynette in adolescents under 18 years of age have not been established. There are no available data.
Novynette and other drugs
The patient should tell their doctor or pharmacist about all the drugs they are currently taking or have recently taken, as well as any drugs they plan to take. The patient should also inform any other doctor or dentist who prescribes any other drug (or pharmacist) about the use of Novynette. Doctors may advise whether additional contraceptive methods should be used (e.g. condoms) and for how long.
Novynette should not be used in patients with hepatitis C and taking medicinal products containing ombitasvir/paritaprevir/ritonavir, dasabuvir, glecaprevir/pibrentasvir, or sofosbuvir/velpatasvir/voxilaprevir, as these drugs may cause abnormal liver function test results in the blood (increased liver enzyme activity). Before starting these drugs, the doctor will prescribe a different type of contraception. Novynette can be started again about 2 weeks after the end of the above-mentioned treatment. See section "When not to use Novynette".
Some drugs may affect the blood levels of Novynette, leading to reduced contraceptive effectivenessand unexpected bleeding. This includes
- drugs used to treat:
- epilepsy (e.g. phenytoin, phenobarbital, primidone, carbamazepine, felbamate, oxcarbazepine, topiramate),
- tuberculosis (e.g. rifampicin, rifabutin),
- HIV infection (protease inhibitors and non-nucleoside reverse transcriptase inhibitors, such as ritonavir, nevirapine, efavirenz, nelfinavir),
- hepatitis C (boceprevir, telaprevir),
- fungal infections (griseofulvin),
- high blood pressure in the blood vessels of the lungs (bosentan),
- herbal products containing St. John's wort (Hypericum perforatum). If the patient wants to use herbal products containing St. John's wort while using Novynette, they should consult their doctor first.
The following drugs may reduce the tolerance of Novynette:
- ketokonazole, itraconazole, fluconazole (used to treat fungal infections);
- macrolide antibiotics, such as clarithromycin, erythromycin (used to treat bacterial infections);
- calcium channel blockers, such as diltiazem (used to treat certain heart diseases and high blood pressure);
- etoricoxib (used to treat arthritis, degenerative joint disease).
Novynette may affect the action of other drugs, such as:
- cyclosporin (a drug used to prevent organ rejection after transplants),
- the antiepileptic drug lamotrigine (may lead to an increased frequency of seizures),
- tizanidine (a drug used to treat muscle spasticity),
- levothyroxine (a drug used to treat hypothyroidism),
- theophylline (a drug used to treat asthma).
Before using any drug, the patient should consult their doctor or pharmacist.
Lab tests
The doctor or laboratory staff should be informed about the use of oral contraceptives, as they may affect the results of some tests.
Pregnancy and breastfeeding
If the patient is pregnant or breastfeeding, thinks they may be pregnant, or plans to have a child, they should consult their doctor or pharmacist before using this drug.
Novynette should not be used when the patient is pregnant. If the patient is pregnant or suspects they may be pregnant, they should stop using Novynette immediately and inform their doctor without delay.
Novynette is not recommended for use during breastfeeding. If the patient is breastfeeding and wants to use oral contraceptives during this time, they should contact their doctor.
Driving and using machines
Novynette can be used while driving and operating machines.
Novynette contains lactose monohydrate
If the patient has been diagnosed with intolerance to some sugars, they should contact their doctor before taking the drug.
3. How to use Novynette
This drug should always be used as directed by the doctor. In case of doubts, the doctor or pharmacist should be consulted.
Each pack of Novynette contains 1 blister pack of 21 coated tablets or 3 blister packs of 21 coated tablets. The special labeling of the blister packs with symbols of consecutive days of the week makes it easier to control the regular use of oral contraceptives.
Each tablet in the pack is marked with a symbol of the day of the week on which it should be taken. One tablet should be taken daily for 21 consecutive days, following the direction of the arrow on the blister pack, until the pack is empty.
After taking all 21 tablets from the blister pack, there is a 7-day break in taking the tablets. During the 2nd or 3rd day of the break, withdrawal bleeding should occur, similar to menstrual bleeding.
The next pack of Novynette should be started on the 8th day (after a 7-day break in taking the tablets), even if the bleeding has not stopped yet. With regular use of Novynette, the start of taking tablets from the next pack will always fall on the same day of the week, and bleeding will occur on the same day of the month.
Tablets should always be taken at the same time.
Taking tablets in the morning (the first thing in the morning) or late in the evening (the last thing before bed) can make it easier to remember to take them regularly.
Tablets should be swallowed whole, with water if necessary.
How to start using Novynette
In the case of not using hormonal contraceptives (in the previous month)
Tablet intake should be started on the first day of the woman's natural menstrual cycle (i.e. on the first day of menstruation). It is allowed to start taking tablets between the 2nd and 5th day, but during the first cycle, additional mechanical contraceptive methods (e.g. condoms) should be used for the first 7 days of tablet intake.
Changing from another combined contraceptive (tablet, vaginal system, transdermal system)
The woman should start using Novynette the next day after taking the last active tablet of the previous oral contraceptive, or at the latest on the first day of the usual break in using the previous contraceptive. Additional contraceptive methods are not required.
If the patient previously used a vaginal system or transdermal system, they should start taking Novynette on the day the system is removed, or at the latest on the day the next application is scheduled. Additional contraceptive methods are not required.
Changing from progestogen-only contraceptives (minipills, injections, implants)
The woman can switch from a progestogen-only tablet at any time (from an implant on the day of its removal or from injections on the day the next injection is scheduled) to Novynette, but in all cases, additional contraceptive methods should be used for the first 7 days of tablet intake.
Use after miscarriage in the first trimester of pregnancy
Tablet intake should be started immediately. Additional contraceptive methods are not required.
Use after childbirth or miscarriage in the second trimester of pregnancy
For breastfeeding women, see section: "Pregnancy and breastfeeding".
The doctor will advise the patient to start taking tablets between the 21st and 28th day after childbirth or miscarriage in the second trimester. If tablet intake is started later, additional mechanical contraceptive methods (e.g. condoms) should be used for the first 7 days of tablet intake. However, if the woman has had sexual intercourse, she should make sure she is not pregnant before starting to use Novynette or wait for her first menstrual period.
Using a higher dose of Novynette than recommended
If an overdose of Novynette occurs, there is no risk of serious health disorders, although nausea, vomiting, or slight vaginal bleeding may occur in young girls. If such symptoms occur, the doctor should be contacted, who will provide appropriate treatment if necessary.
Missing a dose of Novynette
If a dose of Novynette is missed, the following rules should be followed.
If the tablet intake is delayed by less than 12 hours, the contraceptive protection is not reduced. The woman should take the missed tablet as soon as she remembers, even if it means taking 2 tablets at the same time, and then take the next tablets at the usual time.
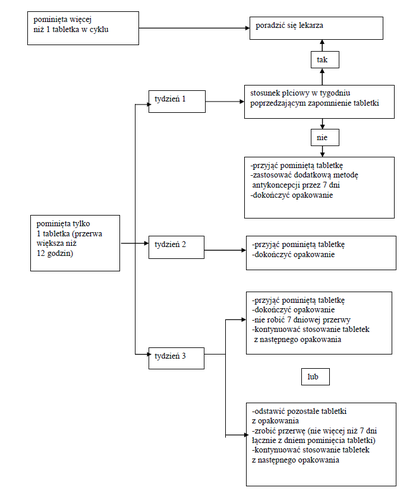
If the tablet intake is delayed by more than 12 hours, the contraceptive protection may be reduced. The more missed tablets, the higher the risk of reduced contraceptive effectiveness. A higher risk of pregnancy exists if a tablet is missed at the beginning or end of the cycle. Please refer to the information provided below (see also the scheme).
More than one missed tablet from the pack
The doctor should be consulted.
In the case of missed tablets, the following two basic rules should be followed:
- 1. The break in continuous tablet intake should never be longer than 7 days.
- 2. It is necessary to take tablets continuously for 7 days to achieve the appropriate inhibition of the hypothalamic-pituitary-ovarian axis.
In accordance with this, in everyday practice, the doctor may provide the following advice:
Week 1
The patient should take the last missed tablet as soon as she remembers, even if it means taking 2 tablets at the same time. Then she should continue taking the tablets at the usual time of day. For the next 7 days, she should use additional mechanical contraceptive methods, e.g. condoms. If sexual intercourse occurred during the 7 days preceding the day the tablet was missed, pregnancy should be considered. The more tablets missed and the closer to the break in tablet intake, the higher the risk of pregnancy.
Week 2
The patient should take the last missed tablet as soon as she remembers, even if it means taking 2 tablets at the same time. Then she should continue taking the tablets at the usual time of day. If the tablets were taken correctly for 7 days preceding the day the tablet was missed, there is no need to use additional contraceptive methods. However, if this was not the case or if the woman missed more than 1 tablet, additional contraceptive methods should be used for 7 days.
Week 3
The risk of reduced contraceptive protection is inevitable due to the upcoming break in tablet intake. However, this can be prevented by adjusting the way the tablets are taken.
Therefore, there is no need to use additional contraceptive methods if one of the two alternative rules below is followed, provided that all tablets were taken correctly during the 7 days preceding the day the tablet was missed. If this is not the case, the first of the two alternative rules should be followed, and additional contraceptive methods should be used for the next 7 days.
- 1. The patient should take the last missed tablet as soon as she remembers, even if it means taking 2 tablets at the same time. Then she should continue taking the tablets at the usual time of day. The next pack of Novynette should be started immediately after finishing the current pack, i.e. without a break between packs. Withdrawal bleeding may not occur until the end of the next pack, but bleeding or spotting may occur during tablet intake.
- 2. The doctor may advise the patient to stop taking the tablets from the current pack. In this case, the patient should take a break from tablet intake for up to 7 days, including the days she missed tablets, and then continue taking the tablets from the next pack.
If the patient misses tablets and withdrawal bleeding does not occur during the first break in tablet intake, pregnancy should be considered.
Using Novynette in case of vomiting or severe diarrhea
If vomiting or severe diarrhea occur within 3-4 hours of taking a tablet, it may not be fully absorbed. In this case, the patient should follow the same rules as for missed tablets described above. If the patient does not want to change their usual way of taking tablets, they should take an additional tablet (tablets) from another pack.
How to delay the occurrence of withdrawal bleeding
If Novynette is taken correctly, withdrawal bleeding will always occur on the same day of the month.
To delay the occurrence of withdrawal bleeding, after finishing one pack of tablets, the patient should continue taking Novynette from the next pack without a break in tablet intake.
Tablet intake can be continued until the end of the second pack. During the use of tablets from the second pack, spotting or bleeding may occur.
Regular Novynette intake should be started after a 7-day break in tablet intake.
To shift the occurrence of withdrawal bleeding to a different day of the week than usual, the next break in tablet intake should be shortened (but never extended) by any number of days. For example, if the first day of bleeding usually falls on a Friday, and it would be more convenient to have it on a Tuesday, i.e. 3 days earlier, the patient should start taking tablets from the next pack 3 days earlier. The shorter the break in tablet intake, the higher the risk that withdrawal bleeding will not occur and that spotting or bleeding will occur during the use of the next pack (similar to delaying the occurrence of withdrawal bleeding).
4. Possible Side Effects
Like all medicines, this medicine can cause side effects, although not everybody gets them.
If side effects occur, especially severe and persistent ones, or changes in health that the patient considers to be related to the use of Novynette, a doctor should be consulted.
A doctor should be contacted immediately if the patient experiences any of the following symptoms of angioedema: facial swelling, tongue and/or throat swelling, and/or difficulty swallowing or hives potentially accompanied by difficulty breathing (see also "Warnings and Precautions").
In all women using combined hormonal contraceptives, there is an increased risk of blood clots in the veins (venous thromboembolism) or blood clots in the arteries (arterial thrombosis). For detailed information on the various risk factors associated with the use of combined hormonal contraceptives, refer to section 2 "Important Information Before Using Novynette".
Frequent (may occur in up to 1 in 10 people):depression, mood changes, headache, nausea, abdominal pain, breast pain, breast tenderness, weight gain.
Uncommon (may occur in up to 1 in 100 people):fluid retention, decreased libido, migraine, vomiting, diarrhea, rash, hives, breast enlargement.
Rare (may occur in up to 1 in 1000 people):hypersensitivity, increased libido, eye irritation due to contact lenses, skin disorders (erythema multiforme, erythema nodosum), abnormal cervical smear, breast discharge, weight loss.
Harmful blood clots in a vein or artery, for example:
- in the leg or foot (e.g., deep vein thrombosis),
- in the lungs (e.g., pulmonary embolism),
- heart attack,
- stroke,
- mini-stroke or transient stroke-like symptoms, known as a transient ischemic attack,
- blood clots in the liver, stomach, and/or intestine, kidneys, or eye. The risk of blood clots may be higher if the patient has any other risk factors (see section 2 for more information on risk factors and symptoms of blood clots).
Reporting Side Effects
If any side effects occur, including those not listed in the leaflet, the doctor, pharmacist, or nurse should be informed. Side effects can be reported directly to the Department of Monitoring of Adverse Reactions to Medicinal Products, Office for Registration of Medicinal Products, Medical Devices, and Biocidal Products, Al. Jerozolimskie 181C, 02-222 Warsaw, Tel.: +48 22 49 21 301, Fax: +48 22 49 21 309, Website: https://smz.ezdrowie.gov.pl
Reporting side effects will help to gather more information on the safety of the medication.
5. How to Store Novynette
The medicine should be stored out of sight and reach of children.
Do not store above 30°C. Store in the original packaging.
Do not use this medicine after the expiry date stated on the packaging. The expiry date refers to the last day of the specified month.
Medicines should not be disposed of via wastewater or household waste. The pharmacist should be asked how to dispose of unused medicines. This will help protect the environment.
6. Package Contents and Other Information
What Novynette Contains
The active substances are ethinylestradiol and desogestrel. One coated tablet contains 20 micrograms of ethinylestradiol and 150 micrograms of desogestrel.
Other ingredients are:
Tablet core: all-rac-α-tocopherol, magnesium stearate, colloidal anhydrous silica, stearic acid, povidone K 30, potato starch, lactose monohydrate, quinoline yellow (E 104).
Coating: propylene glycol, macrogol 6000, hypromellose.
Appearance and Package Contents of Novynette
Pale yellow, round, biconvex tablets with engraved "RG" on one side and "P9" on the other side.
The carton contains 1 blister or 3 blisters of 21 coated tablets.
A cardboard wallet is included in the packaging, in which the blister should be placed.
For more detailed information, the marketing authorization holder or parallel importer should be contacted.
Marketing Authorization Holder in Belgium, Country of Export:
Gedeon Richter Plc., Gyömrői út 19-21, 1103 Budapest, Hungary
Manufacturer:
Gedeon Richter Plc., Gyömrői út 19-21, 1103 Budapest, Hungary
Parallel Importer:
Delfarma Sp. z o.o., ul. Św. Teresy od Dzieciątka Jezus 111, 91-222 Łódź
Repackaged by:
Delfarma Sp. z o.o., ul. Św. Teresy od Dzieciątka Jezus 111, 91-222 Łódź
Belgian, country of export, authorization number: BE339412
Parallel Import Authorization Number: 85/25
Translation of Day Symbols on the Packaging:
Lu/Mo/ma – Monday
Ma/Di/di
- Tu/We/woe - Tuesday Me/Mi/woe - Wednesday Je/Do/don - Thursday Ve/Fr/vrij
- Fr/Fr/vrij - Friday Sa/Sa/zat
- Sa/Su/zon - Saturday Di/Su/zon
- Su/Su/zon - Sunday
Leaflet Approval Date: 05.03.2025
[Information about the trademark]
- Country of registration
- Dosage formTablets, 0.02 mg + 0.15 mg
- ATC codeG03AA09
- Active substance
- Prescription requiredYes
- Marketing authorisation holder (MAH)Gedeon Richter Plc.
- This information is for reference only and does not constitute medical advice. Always consult a doctor before taking any medication. Oladoctor is not responsible for medical decisions based on this content.
- Alternatives to NovinetteDosage form: Tablets, 30 mcg + 150 mcgActive substance: desogestrel and ethinylestradiolManufacturer: mibe GmbH Arzneimittel Sun-Farm Sp. z o.o.Prescription requiredDosage form: Tablets, 20 mcg + 150 mcgActive substance: desogestrel and ethinylestradiolManufacturer: mibe GmbH Arzneimittel Sun-Farm Sp. z o.o.Prescription requiredDosage form: Tablets, 0.15 mg + 0.03 mgActive substance: desogestrel and ethinylestradiolManufacturer: N.V. OrganonPrescription required
Online doctors for Novinette
Discuss questions about Novinette, including use, safety considerations and prescription review, subject to medical assessment and local regulations.
Get Novinette Prescription Online
Fill in a 2-min form
Tell us your symptoms, history, and what medicine you're requesting.
Pick a doctor or let us assign
Choose a specialist or we'll match you with the next available doctor.
Doctor reviews your case
Usually within 30 minutes. They may ask follow-up questions via chat.
Collect from any pharmacy
Electronic prescription sent to your email — valid across Spain.
Frequently Asked Questions
Novinette requires a prescription in Poland. You can check with a doctor online whether this medicine may be appropriate for your situation.
The active ingredient in Novinette is desogestrel and ethinylestradiol. This information helps identify medicines with the same composition but different brand names.
Novinette is manufactured by Gedeon Richter Plc.. Pharmacy brands and packaging may differ depending on the distributor.
Doctors such as Family doctors, Psychiatrists, Dermatologists, Cardiologists, Endocrinologists, Gastroenterologists, Pulmonologists, Nephrologists, Rheumatologists, Hematologists, Infectious disease physicians, Allergists, Geriatricians, Paediatricians, Oncologists may assess whether Novinette is appropriate, depending on your situation and local regulations. You can book an online consultation to discuss your symptoms and possible next steps.
Spain has a well-developed healthcare infrastructure across major cities such as Madrid, Barcelona, Valencia, and Seville. Pharmacies are widely available and operate under strict regulations, ensuring access to prescribed medications.
You can buy Novinette in Madrid, Barcelona, Seville, or Valencia at any local pharmacy with a valid prescription.
To obtain a prescription, you can use Oladoctor:
Other medicines with the same active substance (desogestrel and ethinylestradiol) include Dessette Forte, Dessette, Marvelon. These may have different brand names or formulations but contain the same therapeutic ingredient. Always consult a doctor before switching or starting a new medicine.
